What makes up the sacrum?
The sacrum is the triangular bone just below the lumbar spine. The sacrum has five segments fused together into one large bone. The coccyx or tailbone attaches to the bottom of the sacrum.
The sacrum forms the base of the spine and the center of the pelvis. The sacrum transmits the weight of the body to the pelvic girdle. It is shorter and wider in the female than in the male. Its name means sacred bone.
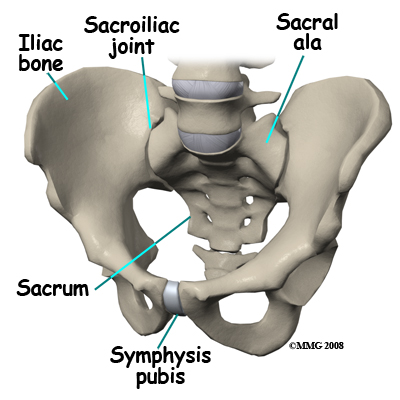
At the top of the sacrum there are wings from each side called the sacral ala. At the ala, the sacrum fits between the two halves of the pelvis. These pelvic bones are called the iliac bones. This is where the sacroiliac joints are formed. Most everyone has two dimples in their low back where the sacroiliac joints form. These three bones of the pelvis, the sacrum and the two iliac bones, make a ring.
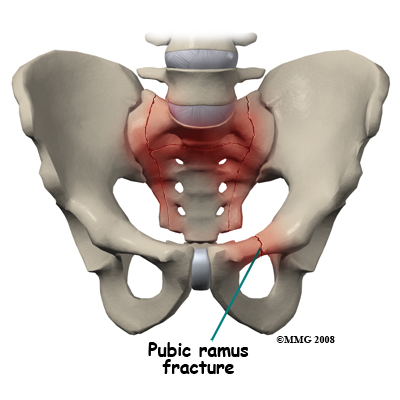
Each of the iliac bones has projections called the pubic rami. They meet together in the front of the pelvis, forming a joint called the symphysis pubis. The iliac bones also contain the cup or socket for the hip joint.
Nerves that leave the spine in the area of the sacrum help control the bowels and bladder and provide sensation to the crotch area.
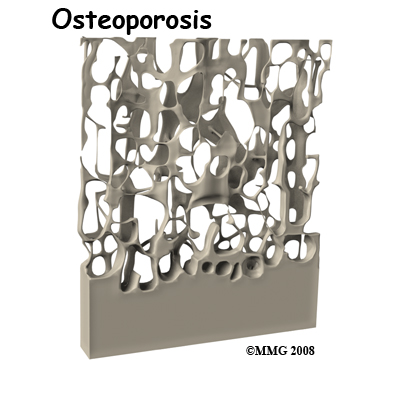
There are three types of bone, woven bone, cortical bone, and cancellous bone. In adults, woven bone is found where there is a broken bone that is healing (callus formation). It can also be found with hyperparathyroidism and Paget's disease. It is composed of randomly arranged collagen strands. It is normally remodeled by the body and replaced with cortical or cancellous bone.
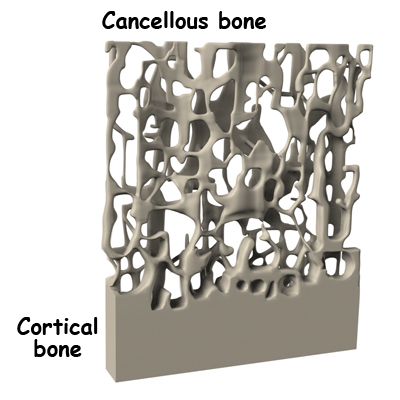
Cortical bone is called compact or lamellar bone. It forms the inside and outside tables of flat bones and the outside surfaces of long bones. It is dense and makes up 80 percent of our bone mass. The radius (wrist bone), skull, and long bones are made of cortical bone.
Cancellous bone is also called trabecular bone. It lies between the cortical bone surfaces. It is the inner supporting structure and is spongy. It makes up 20 percent of our bone mass. Normal cancellous bone is always undergoing remodeling on the inside surfaces of bone. Cancellous bone is found in the hip, spine, and femur.
The three main cells that form and shape bones are osteoblasts, osteocytes, and osteoclasts. Osteoblasts are bone-forming cells. When calcium is deposited in the cells, they make bones strong and hard. Osteocytes are mature osteoblasts trapped within the bone. Osteoclasts are bone-resorbing cells. They dissolve bone surfaces by releasing a chemical called an enzyme. Their activity is in part controlled by hormones in the body.
It is normal for bones to have mini fractures from everyday wear and tear. They are healed by ongoing bone remodeling. Bone remodeling occurs in 120 day cycles. Normal bone has a balance of clearing away old bone and formation of new bone. Osteoclasts resorb or clear away the damaged bone for the first 20 days. Bone is then formed by osteoblasts over the last 100 days.
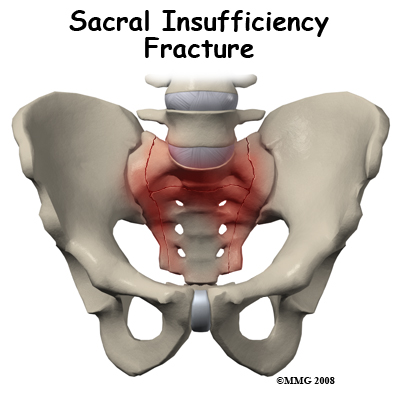
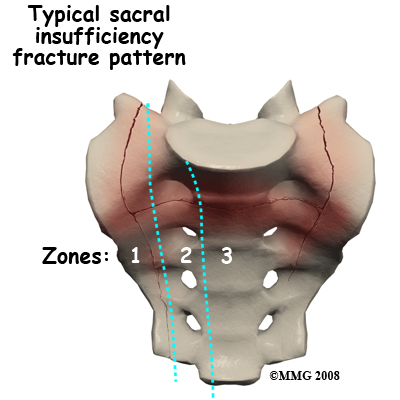
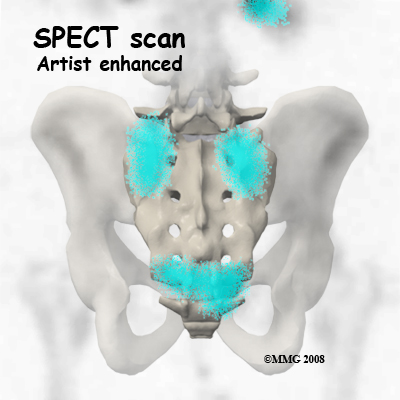
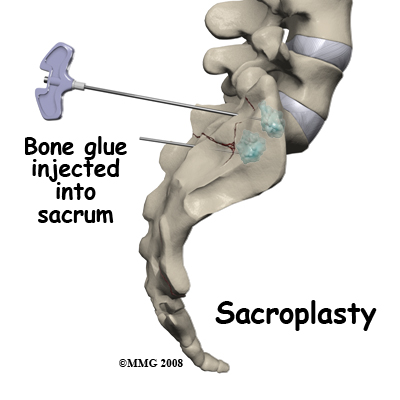
Sacral insufficiency fractures usually are parallel to the spine. They are most often in the ala, just beside the sacroiliac joint. At times there is also a transverse fracture that connects insufficiency fractures when they occur on both sides of the sacrum. The fracture lines then create an "H" pattern. Sacral fractures are classified into three zones, zone 1, zone 2, and zone 3. If the fracture involves just the ala, there is usually not a risk for nerve damage.
Related Document: Next Step Physio's Guide to Lumbar Spine Anatomy